

Suite 03-06 Gleneagles Medical Centre
6 Napier Road Singapore 258499

 Professor Merserkinger - father of Endoscopic Sinus Surgery with Dr Stanley in Graz, Austria 1991.
Professor Merserkinger - father of Endoscopic Sinus Surgery with Dr Stanley in Graz, Austria 1991.  Hands-on Laboratory Endoscopic Sinus Surgery Course, Graz, Austria
Hands-on Laboratory Endoscopic Sinus Surgery Course, Graz, Austria Outpatient Endoscopy - Flexible
Outpatient Endoscopy - Flexible Diagnostic Rigid Nasoendoscopy
Diagnostic Rigid Nasoendoscopy Thorough evaluation of CT Scans are essential
Thorough evaluation of CT Scans are essential Endoscopic Sinus Surgery
Endoscopic Sinus Surgery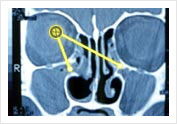 Blocked Osteo-Meatal Complex Before Surgical Treatment of Chronic Sinusitis
Blocked Osteo-Meatal Complex Before Surgical Treatment of Chronic Sinusitis Before operation
Before operation Scan before operation Mucocele in Ethmoid
Scan before operation Mucocele in Ethmoid Endoscophic Drainage of Ethmoidal Mucocele during and end of operation
Endoscophic Drainage of Ethmoidal Mucocele during and end of operation Endoscophic Drainage of Ethmoidal Mucocele during and end of operation
Endoscophic Drainage of Ethmoidal Mucocele during and end of operation CT Scan after operation
CT Scan after operation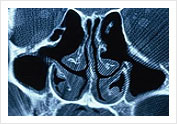 Post-operative FESS cavity on CT Scan
Post-operative FESS cavity on CT Scan Endoscopic View of Ethmoidal Cavity after FESS operation
Endoscopic View of Ethmoidal Cavity after FESS operation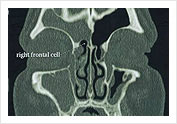 Frontal Cell causing Frontal Sinusitis – Suitable for Balloon Sinuplasty
Frontal Cell causing Frontal Sinusitis – Suitable for Balloon Sinuplasty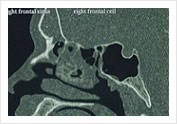 Frontal Sinusutus – Suitable for Balloon Sinusplasty from Obstructing Frontal Cell
Frontal Sinusutus – Suitable for Balloon Sinusplasty from Obstructing Frontal Cell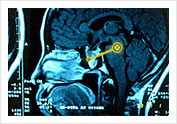 Pituitary tumour eroding the sphenoid sinus
Pituitary tumour eroding the sphenoid sinus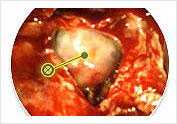 Intra-operative Transphenoidal view of tumor
Intra-operative Transphenoidal view of tumor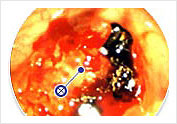 Post-operative view in the clinic 1 week after surgery
Post-operative view in the clinic 1 week after surgery Grasping Forcepes
Grasping Forcepes Through Cutting Forcepes
Through Cutting Forcepes
 Tri-Cut Blades
Tri-Cut Blades Frontal Recess Instrument – Micro Debride
Frontal Recess Instrument – Micro Debride Fusion ENT Navigation System with EM Tracking Blade
Fusion ENT Navigation System with EM Tracking Blade

